Indications for a spinal ultrasound study in newborns
All the conditions that may be associated with closed spinal dysraphism are indications for performing a spinal ultrasound study as a screening tool in newborns.
They include[1,3]:
- Midline cutaneous stigmata of the back (sacral dimple,
particularly if located further than 2,5 cm from the anus; hemangiomatous lesion; hairy patches; skin tags);
- Soft-tissue mass of the back;
- Congenital abnormalities:
- Genitourinary malformations
- Anorectal malformations
- Sacral abnormalities.
Specifically at our institution,
these exams are only performed in newborns whose obstetric ultrasound studies did not reveal significant changes,
otherwise MRI is the chosen imaging study.
Normal findings ( Fig. 1,
Fig. 2)
Spinal ultrasound study is performed in both sagittal and axial planes along the midline,
with the newborn in prone position.
The spinal cord appears as a hypoechoic tubular structure with a hyperechoic center representing the central canal – the central echo complex.
The caudal extremity of the spinal cord corresponds to the conus medullaris,
whose tip is usually located in the level between L1 and L2 in healthy newborns.
It should not lie below the L2-L3 disk space[1,4].
The conus medullaris continues into a hyperechoic cordlike structure,
the filum terminale,
which is surrounded by echogenic linear structures representing the roots of the cauda equina.
The filum terminale thickness should not overcome 2 mm.
The normal spinal cord and cauda equina demonstrate pulsatile movements,
which may be assessed with M-mode study[5](Fig. 3).
The subarachnoid space surrounding the spinal cord appears anechoic,
since it is filled with cerebrospinal fluid.
Limiting the subarachnoid space,
ventrally and dorsally,
there is an echogenic line corresponding to the arachnoid-dura mater complex,
which coincides with the border of the spinal canal.
Ventral to the spinal cord,
the vertebral bodies are also identified and appear as echogenic structures[1].
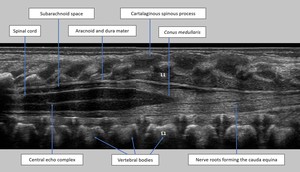
Fig. 1: Normal anatomy of the distal spinal canal and its content in a 7-day-old newborn - sagittal ultrasound image. The L1 vertebra is indicated.
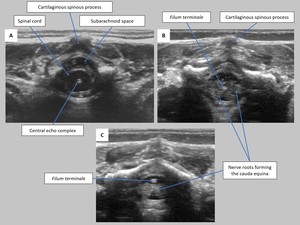
Fig. 2: Normal anatomy of the lumbar spinal canal and its content – axial ultrasound images (A obtained at a higher level than B, B at a higher level than C).
Normal variants
Normal variants are commonly found in spinal ultrasound studies.
Its recognition is fundamental in order to prevent its misinterpretation as pathologic findings and unnecessary additional evaluations.
Transient dilation of the central canal (Fig. 4)
The spinal cord may present a slight dilation of the central canal during the first weeks of life after birth.
This seems to be an incidental finding in healthy newborns[5].
Ventriculus Terminalis and Filar Cyst
Although some authors refer to both as synonymous,
others distinguish these two entities[3,5]
Ventriculus Terminalis corresponds to a small distension of the distal lumbar central canal of the spinal cord,
above the tip of the conus medullaris (Fig. 5).
To be considered a simple variant,
it should be smaller than 5 mm and stable over time.
It results from an incomplete fetal regression of the embryonic terminal ventricle in the conus medullaris[3].
Filar Cyst refers to a well-defined and fusiform cystic structure located in midline,
within the filum terminale,
immediately below the conus medullaris (Fig. 6).
Two principal hypotheses explain its origin.
One is that it may be a pseudocystlike structure resulting from the normal arachnoid reflections.
The other one is that it is a true cystic embryonic remnant[3].
Pseudosinus Tract
Pseudosinus tract is a common normal variant found in spinal ultrasound studies.
It is characterized by a residual cord of fibrous tissue extending from the coccyx to the base of a skin dimple.
In ultrasound imaging it is seen as a hypoechoic cordlike structure arising from the tip of the coccyx[3] (Fig. 7).
Dysmorphic Coccyx (Fig. 8)
The shape and angulation of the coccyx are quite variable.
In some cases,
its tip is angulated in a way that simulates a palpable mass during the physical examination[3].
Pathologic conditions
Tethered spinal cord
Tethered spinal cord may be associated with both open and closed spinal dysraphisms,
and results from incomplete regressive differentiation and failed involution of the terminal cord.
The filum terminale and the nerve roots are abnormally anchored,
leading to the dorsal fixation of the spinal cord[4].
In ultrasound imaging two main features are seen:
- The conus medullaris is in a low-position,
below the L2-L3 disk space;
- The spinal cord and nerve roots show lack of movement in M-mode scanning[5].
Fatty Filum or Filar Lipoma
Fatty filum or filar lipomas result from a minor anomaly in secondary neurulation,
leading to persistence of dedifferentiated fatty tissue within the filum terminale[4].
Fatty filum may be considered a normal variant if it is an isolated finding in a filum with normal thickness (2 mm or less).
It is seen as an increase of echogenicity within the filum (Fig. 9).
When associated with other anomalies,
such as tethered spinal cord,
constitutes a pathologic finding.
Spinal Lipomas (with a dural defect) – Lipomyelocele and Lipomyelomeningocele
Lipomyelocele and lipomyelomeningocele result from a failure in primary neurulation whereby mesenchymal tissue fills the neural tube and differentiates into fat[2,5].
They occur predominantly in the lumbosacral region.
At clinical examination,
a subcutaneous fatty mass above the intergluteal crease is seen.
The location of the interface between the neural tissue and the lipoma is one of the main features distinguishing both entities: in lipomyelocele,
the interface lies within the spinal canal; in lipomyelomeningocele,
the interface lies outside of the spinal canal[2].
Intradural lipoma
This type of lipoma is located within the dural sac,
along the dorsal midline.
They are more frequent in the lumbosacral region and often associated with tethered spinal cord.
Spinal ultrasound depicts an intradural hyperechogenic mass attached to the spinal cord [2].
Dermal sinus tract
Dermal sinus is caused by an incomplete disjunction between the superficial and the neural ectoderm at a focal point[5].
It consists of an epithelial lined tract that connects neural tissue or meninges to the skin surface,
most frequently located in the lumbosacral region.
At physical examination,
it manifests as a midline dimple,
often associated with other cutaneous findings (hairy nevus,
hyperpigmented area or capillary hemangioma)[2].
Sonography may depict a hypoechoic tract extending from the spinal cord to the skin (Fig. 10).
Meningocele
In this closed spinal dysraphism,
there is a herniation of spinal meninges (dura and arachnoid mater) through a vertebral defect.
The hernial sac only contains cerebrospinal fluid.
In ultrasound imaging,
meningoceles appear as subcutaneous cystic dilated subarachnoid spaces[1,2].
Terminal Myelocystocele
This entity is characterized by an association of posterior spinal defect,
meningocele,
hydromyelia and a large terminal syrinx.
The terminal syrinx herniates into a posterior meningocele and communicates with the central canal[2,5].
Diastematomyelia
Diastematomyelia is characterized by the sagittal division of the spinal cord into two symmetrical or asymmetrical hemicords.
The length of separation is variable and the lumbar segment of the spinal cord is frequently affected.
At physical examination,
patients usually present with cutaneous stigmata on the back.
Ultrasound imaging in the axial plane demonstrate the presence of two hemicords[5].
Caudal Regression Syndrome
Caudal regression syndrome represents a spectrum of anomalies of the caudal region,
ranging from isolated partial agenesis of the coccyx to lumbosacral agenesis[4].
It may be associated with other malformations such as anal imperforation,
genitourinary anomalies,
pulmonary hypoplasia or limb anomalies[1].
Patients may be categorized into two groups according to the level and configuration of the conus medullaris.
In type 1,
the conus medullaris has a high position,
terminating above the level of L1,
and presents a blunt-ended shape.
In type 2,
the conus medullaris is elongated and tethered,
assuming a low position[5].
Hydromyelia and Syringomyelia
Hydromyelia refers to dilation of the central canal of the spinal cord.
Syringomyelia refers to the presence of a paracentral cystic cavity – syrinx – related to laceration of the ependymal lining of the central canal and consequent “leaking” of cerebrospinal fluid into the spinal cord parenchyma (Fig. 11).
These two conditions may result from changes in cerebrospinal fluid circulation or consist in variants of dysraphic malformations[5].
Vertebral posterior arch fusion defects (Fig. 12)
Isolated vertebral posterior arch fusion defects are a mild form of closed spinal dysraphism,
consisting of unfused spinous processes,
laminae or both.
This condition is relatively frequent and commonly seen as an incidental finding,
although it may be associated with a tethered spinal cord.
Transitional levels of the spine,
particularly the L5 and S1 segments,
are most commonly involved[6].


.")

.")
.")
 and axial (B) ultrasound images show a midline, fusiform, cystic collection (arrows) below the conus medullaris.")
 extending from the tip of coccyx (asterisk) to the skin dimple (black arrow). Note the hypoechoic appearance of the coccyx due to its cartilaginous nature.")
.")
. Its maximum thickness was 2 mm. There were no additional findings, whereby, in this case, it was regarded as a normal variant.")
. Axial (B) and sagittal (C) ultrasound images display a hypoechoic tract (arrows) extending from the spinal canal to the cutaneous surface at the skin tag (asterisk indicates the external opening of the sinus tract at the skin tag). Note that the tip of the conus medullaris lies at the L3 level (C), a little lower than normal.")
- within the dorsal spinal cord (arrowheads). The quality of ultrasound assessment was impaired by child's age due to progressive ossification of the posterior spinous elements.")
